A new Ebola outbreak is unfolding right now, and this one is different from the ones you may remember. On May 15, 2026, the Democratic Republic of the Congo (DRC) officially declared an outbreak in its northeastern Ituri Province. Within days, cases had crossed the border into Uganda’s capital Kampala. By May 17, the World Health Organization declared it a Public Health Emergency of International Concern (PHEIC), the highest level of global health alarm.
As of May 27, 2026, more than 1,200 suspected and confirmed cases and at least 264 deaths have been reported. The outbreak is still growing.
What Makes This Outbreak Different
Most people associate Ebola with the Zaire strain, the one responsible for the catastrophic 2014–2016 West Africa epidemic and the large 2018–2019 DRC outbreak. For that strain, there is an approved vaccine (rVSV-ZEBOV) and approved treatments. This outbreak is caused by a different species entirely: Bundibugyo virus.
Bundibugyo is rarer. This is only the third time it has been implicated in a known outbreak. It was first identified less than 20 years ago in western Uganda. And critically, as of today, there is no approved vaccine and no approved treatment for Bundibugyo. Scientists and international health agencies are urgently working to test candidate therapies, but nothing is licensed yet. This makes the current outbreak significantly more difficult to manage than previous ones.
The outbreak is also happening in a deeply challenging context: active armed conflict in eastern DRC, a large humanitarian crisis, heavy cross-border population movement, dense urban and semi-urban areas, and limited diagnostic capacity. PCR test kits specific to Bundibugyo are in short supply, which slows case confirmation and contact tracing, the two most critical tools for stopping any Ebola outbreak.
What Is Ebola, and How Does It Work?
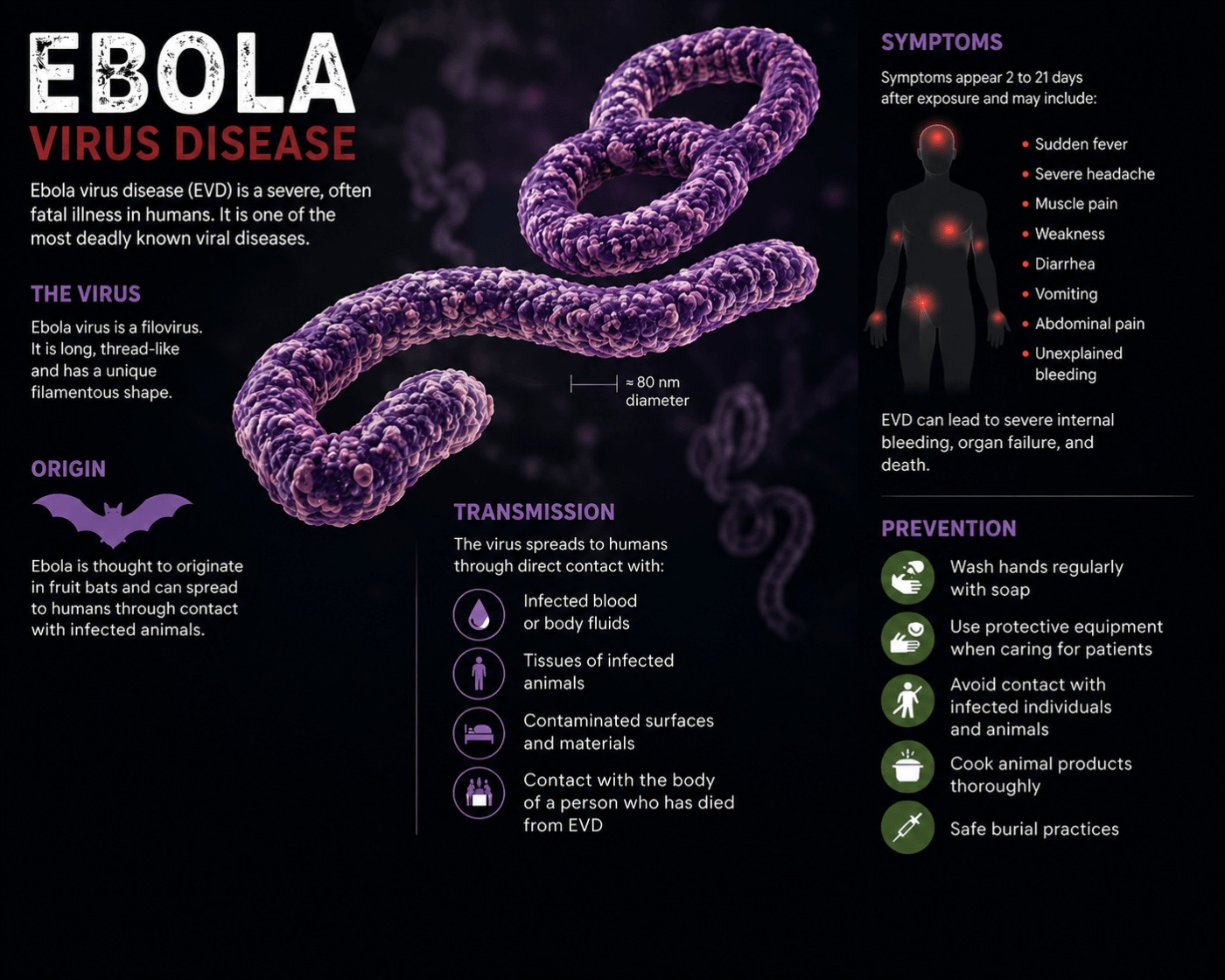
Ebola disease is caused by a family of viruses called ebolaviruses, which are found naturally in sub-Saharan Africa. Fruit bats are believed to be the primary animal reservoir, the species that carries the virus without becoming ill. Occasionally, the virus “spills over” into humans, either through contact with an infected animal or its bodily fluids, and from there it can spread from person to person.
Once inside the human body, the virus attacks multiple organ systems simultaneously. It causes what is known as a viral hemorrhagic fever, though not all patients experience visible bleeding. The disease typically progresses in two phases:
Early “dry” phase: Fever, headache, severe fatigue, muscle aches, and sore throat. These symptoms are non-specific and easy to mistake for malaria, typhoid, or flu, which is part of what makes early detection so difficult.
Later “wet” phase: Vomiting, diarrhea, and in some cases internal or external bleeding. Patients can deteriorate rapidly at this stage. The average incubation period from exposure to symptoms is 8 to 10 days, though it can range from 2 to 21 days.
Crucially, a person is only contagious once symptoms appear. Ebola does not spread through the air. You cannot contract it by passing someone on the street or being in the same room as an infected person who is not yet symptomatic.
How Does It Spread?
Ebola spreads through direct contact with the blood or bodily fluids of a symptomatic infected person, or with contaminated objects such as needles, bedding, or medical equipment. The most common transmission routes are:
- Caring for a sick family member without protective equipment
- Exposure in healthcare settings without proper infection control
- Handling the body of someone who died from Ebola (funeral and burial practices are a significant transmission risk in affected communities)
- Contact with infected animals, though this is rare
Healthcare workers and family caregivers carry the highest risk. The virus can also persist in the body of a survivor, particularly in semen, for weeks to months after recovery, which can lead to sexual transmission even after a person appears well.
What Is the Risk for People Outside DRC and Uganda?
For the vast majority of people in Europe, North America, and elsewhere, the current risk is very low. Ebola does not spread easily in settings with functioning healthcare infrastructure, running water, and robust infection control. The CDC currently rates the risk to the United States as low, though it has issued a Level 3 Travel Health Notice (avoid non-essential travel) for DRC and a Level 1 Notice (practice usual precautions) for Uganda.
Enhanced health screening is in place at airports for travelers arriving from affected regions. The US, EU, and other governments are coordinating with airlines and port-of-entry officials to identify and manage anyone who may have been exposed.
That said, the fact that cases have already appeared in Kampala, a major international hub, is a reminder that in a connected world, no outbreak stays local forever. Vigilance matters.
How to Protect Yourself
If you are not in an affected region: Stay informed through official sources (CDC, WHO). There is no need for alarm, but awareness is useful. Monitor travel advisories before any trip to Central or East Africa.
If you are traveling to DRC, Uganda, or surrounding areas:
- Avoid contact with sick people and with anyone who has died from unknown causes
- Do not handle or consume bushmeat (wild animals)
- Avoid contact with bats and non-human primates
- Wash hands frequently and thoroughly with soap and water or alcohol-based hand sanitizer
- Seek medical attention immediately if you develop fever, fatigue, or other symptoms within 21 days of potential exposure, and inform healthcare workers of your travel history
If you are a healthcare worker or aid worker in an affected area:
- Use full personal protective equipment (PPE) at all times with suspected or confirmed cases
- Follow strict infection prevention and control (IPC) protocols
- Ensure safe and dignified burial practices
- Participate in daily contact monitoring and report symptoms immediately
How Is the Outbreak Being Managed?
Without an approved vaccine or treatment for Bundibugyo, the response relies entirely on proven public health fundamentals: find cases early, isolate them quickly, trace every contact, and protect healthcare workers. WHO, MSF (Doctors Without Borders), the CDC, and many other international partners are on the ground scaling up these efforts.
Contacts of confirmed cases are monitored daily for 21 days, the maximum incubation period. Anyone who develops symptoms is immediately quarantined. Safe burial teams are managing the high-risk process of handling the deceased. Community engagement is a critical part of the response: outbreaks are controlled fastest when local communities understand what is happening and trust the response.
Clinical trials for candidate Bundibugyo-specific treatments and a ring vaccination strategy using available experimental vaccines are being explored. History gives some reason for optimism: every previous Ebola outbreak, including some that seemed uncontrollable at first, has eventually been brought to an end.
A Final Word
Ebola is frightening, partly because of its severity and partly because of how it has been portrayed in popular culture. But it is not a mystery virus, and the science of how to stop it is well understood. What makes outbreaks like this one so difficult is not the biology, it is the context: war, poverty, displacement, and under-resourced health systems.
The best thing most of us can do right now is stay informed, trust verified sources, and support the organisations working on the ground. The worst outcomes in outbreak history have always been driven by fear, misinformation, and delayed response. The best outcomes have come from transparency, coordination, and community trust.
This is a serious situation. It is also one the world knows how to face.
Key sources and further reading:
- WHO situation page: Ebola Outbreak DRC 2026
- CDC outbreak summary: CDC Ebola Situation Summary
- CDC FAQ on Bundibugyo: Ebola and Bundibugyo Virus FAQ
- MSF on the Bundibugyo challenge: Why This Outbreak Is Different
- ECDC rapid risk assessment: ECDC Risk Assessment

Leave a comment